
Picture it: A health system announces a bold initiative to close disparities in surgical outcomes. There’s a press release. A town hall. A task force with an impressive name and a longer list of attendees. Twelve months later, the data hasn’t moved. The task force has met six times. The co-chairs have changed twice. And when you ask who owns the work — truly owns it, with authority and budget — the room goes quiet.
Sound familiar?
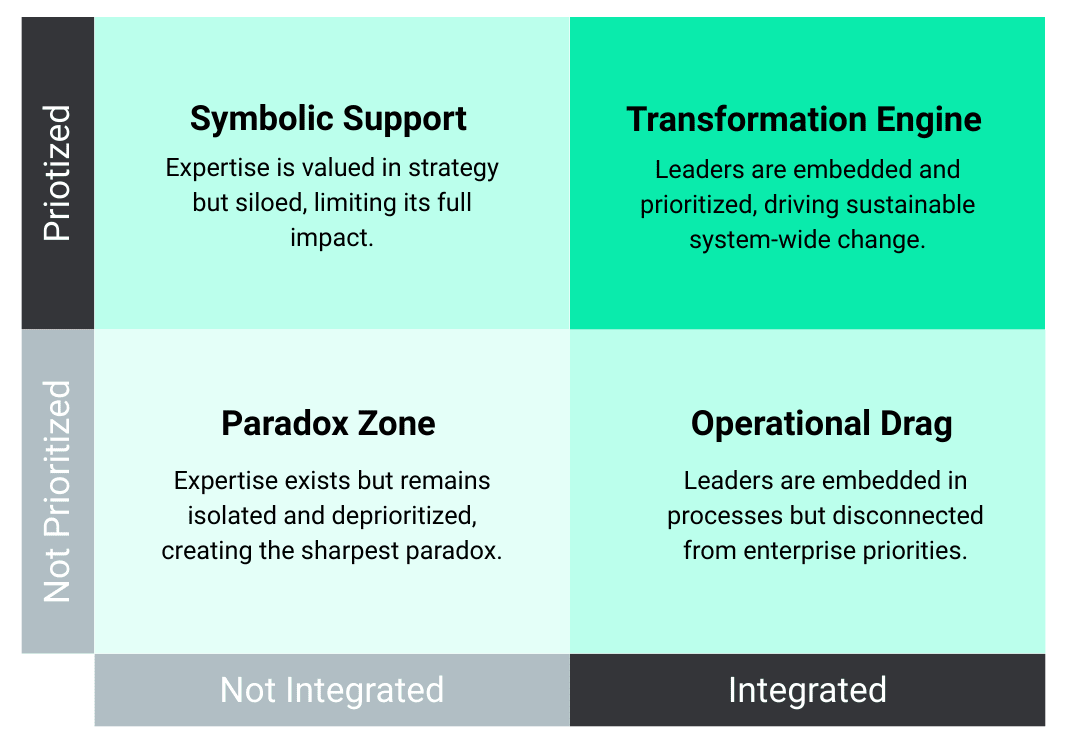
This is not a story about bad leadership. It’s a story about a structural mismatch that plays out in health systems across the country, quietly, repeatedly. The gap isn’t between intention and values. It’s between commitment and infrastructure. In The Leadership Paradox: A Guide to Reimagining Equity in a Changing Healthcare Landscape, we describe this gap more precisely as a tension between prioritization and integration — two forces that determine whether expertise actually drives outcomes or quietly stalls within the system.
The reality is, most organizations don’t lack expertise. They lack alignment.
The tension most organizations refuse to name is this: we have learned to make announcements at the speed of press releases, but we have not learned to build operational capacity at the speed of our ambitions. Health systems and organizations are extraordinarily skilled at declaring priorities. They are far less skilled at engineering the workflows, accountability structures, and resource allocation required to sustain them. Equity work — which requires long-cycle, embedded, cross-functional effort — is particularly vulnerable to this mismatch. It asks the most of an organization’s operational discipline at exactly the moment when that discipline is tested by competing pressures, political headwinds, and leadership turnover.
Change The Frame
The insight that changes the frame: sustainable progress on health equity is not primarily a leadership will problem — it is a systems design problem. This is exactly the gap we see across the ODLC network — organizations with strong commitment, but inconsistent infrastructure to translate that commitment into measurable outcomes. Increasingly, leaders are asking not what we should prioritize, but how we operationalize what we’ve already said matters.
When outcomes don’t improve, we tend to ask whether leaders are committed enough. This is a very common misstep! The more useful question is whether the system has been structurally wired to succeed. Does the work have a named owner with real authority and a dedicated budget, or does it live as an add-on to someone’s already-full role? Is it integrated into the quality infrastructure — tied to patient safety metrics, value-based care targets, and operational dashboards — or is it siloed as a standalone “initiative” that runs parallel to how the organization actually operates? A commitment embedded in culture looks fundamentally different from a commitment embedded in a PowerPoint.
For organizations looking to move from intention to execution, structured assessment can be a powerful starting point. Tools like the Dynamize Health Equity Leadership Index (ELI) were designed to help leaders map where equity is truly embedded versus where it remains aspirational — across governance, operations, and accountability structures.
Translation to Practice
In practice, this means senior leaders need to conduct an honest audit—not of their stated values, but of their operational architecture.
- Identify which equity-focused goals are integrated into existing governance structures and which are floating outside them.
- Examine whether the people accountable for outcomes have the tools, time, and authority to act.
The most durable progress comes from organizations that stopped treating equity as a program and started treating it as a quality imperative — subject to the same rigor, resource investment, and accountability that governs everything else that matters to the institution.
This kind of audit doesn’t happen organically — it requires a shared language, a clear framework, and leaders who are trained to see both the clinical and operational dimensions of the work. That’s where leadership development becomes essential, not optional.
Through the Transformative Value-Driven Care Leadership Certificate, we focus specifically on this intersection — helping clinicians and executives build the skills to align equity, quality, and financial performance into one coherent strategy.
The organizations that are making measurable progress are not the ones with the most visible commitments — they are the ones quietly building the infrastructure to sustain them. Increasingly, those leaders are seeking spaces to test ideas, share strategies, and learn from peers navigating the same complexity.
That is the role ODLC was built to play.
The hardest thing to build in any health system isn’t consensus — it’s infrastructure. And until we stop mistaking the announcement for the action, we will keep wondering why the data doesn’t move.
A strategy without an owner is just a document.
An equity commitment without infrastructure is just a press release.
ODLC Leadership Takeaways:
Name the owner.
Every health equity goal needs a single accountable leader with explicit authority, a defined budget, and a seat at the table where operational decisions are made—not a committee with diffuse responsibility and no decision-making authority.
Integrate, don’t isolate.
Equity work that lives outside your quality, safety, and value-based care infrastructure will always be vulnerable to deprioritization. Embed it into the systems that govern how your organization actually runs.
Audit your architecture, not your intentions.
When outcomes stall, resist the impulse to question commitment. Instead, examine the structural conditions: Does the work have the operational support it needs to succeed?
Where to Go from Here:
- Explore how your organization’s infrastructure stacks up → Equity Leadership Index (ELI)
- Build leadership capability to operationalize this work → Dynamize Health + Cornell Certificate Programs
- Join a network of leaders doing this in real time → ODLC Membership
