
There is a particular kind of meeting every healthcare leader knows.
You are sitting in a conference room, or more likely on a screen with twelve boxes and three cameras off, listening to an update on work that everyone agrees matters. The data points are there. The team is there. The need is obvious. And, somehow, the next step is still not a decision.
It is “alignment.”
It is “executive sponsorship.”
It is “waiting for the right window.”
And listen, I believe in alignment. In healthcare, we cannot move every meaningful thing through force of personality and vibes. Governance matters. Strategy matters. Stewardship matters. But there is a difference between building alignment and hiding inside it. There is a difference between wise sequencing and organizational stalling. There is a difference between needing approval and needing reassurance.
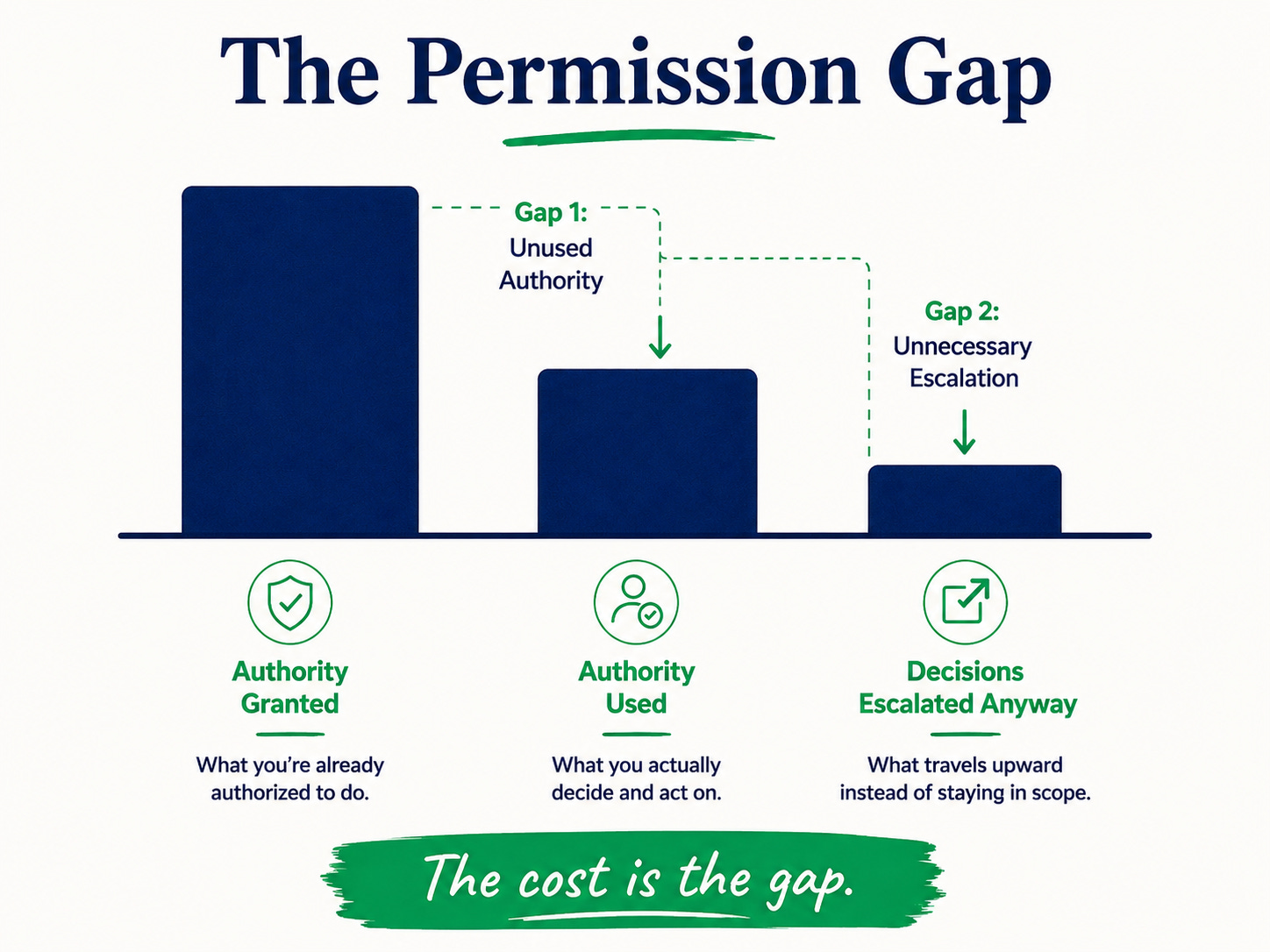
That difference is what I call the permission gap.
The permission gap is the space between the authority a leader has already been given and the authority they are actually using. It shows up when a senior leader escalates decisions already within their scope. It shows up when a team waits for sponsorship before making a change they were already empowered to make. It shows up when the safest move becomes “let me check,” even when nobody actually asked us to check.
And in this moment, that gap is getting wider.
As we have discussed in previous articles, the gap is widening because the climate has made everyone more cautious. Language is being scrutinized. Budgets are tighter. Public narratives are louder. Leaders are trying to read the room, protect their teams, preserve momentum, and avoid unnecessary exposure.
That caution is understandable. But caution becomes costly when it quietly migrates into work that was never actually controversial.
Improving access reliability is not controversial. Reducing preventable gaps in outcomes is not controversial. Building better processes for referrals, mentorship, patient access, and team communication is not controversial.
That is healthcare leadership.
We are misdiagnosing the constraint. We assume the constraint is permission, when it is usually clarity about how much permission we already have. The Harvard Business Review has been writing about decision rights and the pathology of escalation by default for over a decade. Becker’s keeps documenting the same dynamic inside hospital governance research.
The pattern is consistent across health systems: a meaningful share of decisions gets pushed upward that the leader was already authorized to make. In the current climate, that pattern has not improved. The political headwinds have made everyone slightly more cautious, and that caution has quietly shifted from genuinely controversial work to work that was never controversial to begin with.
A Practical Audit of Unused Authority
Here are three small self-audits you can do today.
- First, audit your escalations. List the last five decisions you pushed upward. For each one, ask: Did this actually require sign-off, or did I escalate it because I wanted someone else to share the risk of being wrong?
That question may sting a little. Let it.
- Second, walk your scope. Look at what you already control: meeting agendas, selection criteria, referral patterns, promotion conversations, mentorship structures, onboarding practices, dashboards, workflows, team norms, and follow-up expectations. Then identify two changes you can make this quarter without a single additional approval.
Tip: Make them real enough to matter and small enough to move.
- Third, name what is sitting unmade. Look at the decisions sitting in your inbox, your notes app, your draft agenda, or that “circle back” folder in your brain. Which ones are waiting on an external signal? And here is the more important question: Is that signal actually coming?
Many of you have been holding the line through a season of political noise, and the discipline of holding it has cost you something real. The work that does not require external validation is also the work nobody can take from you when the language of the field shifts, when budgets compress, when the public attention moves on. You hold more authority than the room is letting you recognize. Use it. Our network is doing this work together, one leadership move at a time.
Leadership Takeaways
For our ODLC community, this is not a call to be reckless. We know the room. We understand context, governance, timing, and politics. But we also know the difference between strategic patience and learned deference.
Strategic patience says, “This decision has real implications, and I need the right people at the table.” Learned deference says, “I technically own this, but I am waiting for someone above me to make it feel safer to act.”
Those are not the same.
So this week, ask yourself:
What am I allowed to move that I have been treating as if it still needs permission?
What decision have I escalated that belongs back in my hands?
What part of the work can I build into the system before another quarter disappears?
Resource Connection
This is part of why we built the Dynamize Health Strategic Change and Innovation Leadership Certificate with Cornell. A good deal of leadership work is about moving real decisions through complex systems.
The courses are designed for exactly this kind of moment: leading change when conditions are imperfect, building coalitions without waiting forever, navigating resistance, testing new ideas, and turning strategy into operating habits.
For leaders working inside the permission gap, the goal is not to become louder. It is to become clearer, more strategic, and more practiced at using the authority already in hand.
