
There is a version of this story I hear across healthcare all the time: a clinical team is trying to improve outcomes, a quality team is tracking variation, a community health team is building partnerships, a data team is refining dashboards, a workforce team is trying to address retention and burnout, and a med tech partner is introducing a solution that could improve efficiency or access.
Everyone is working. Everyone is committed. Everyone can point to meetings, metrics, updates, pilots, and progress. And still, somehow, the work does not fully move.
Now, this is not because people are apathetic. It is not even because the mission is unclear. Nor is it because the organization lacks intelligence, innovation, or good intent. Often, the work stalls because the system has made it easier for leaders to solve connected problems separately.
That is the hidden cost of siloed leadership.
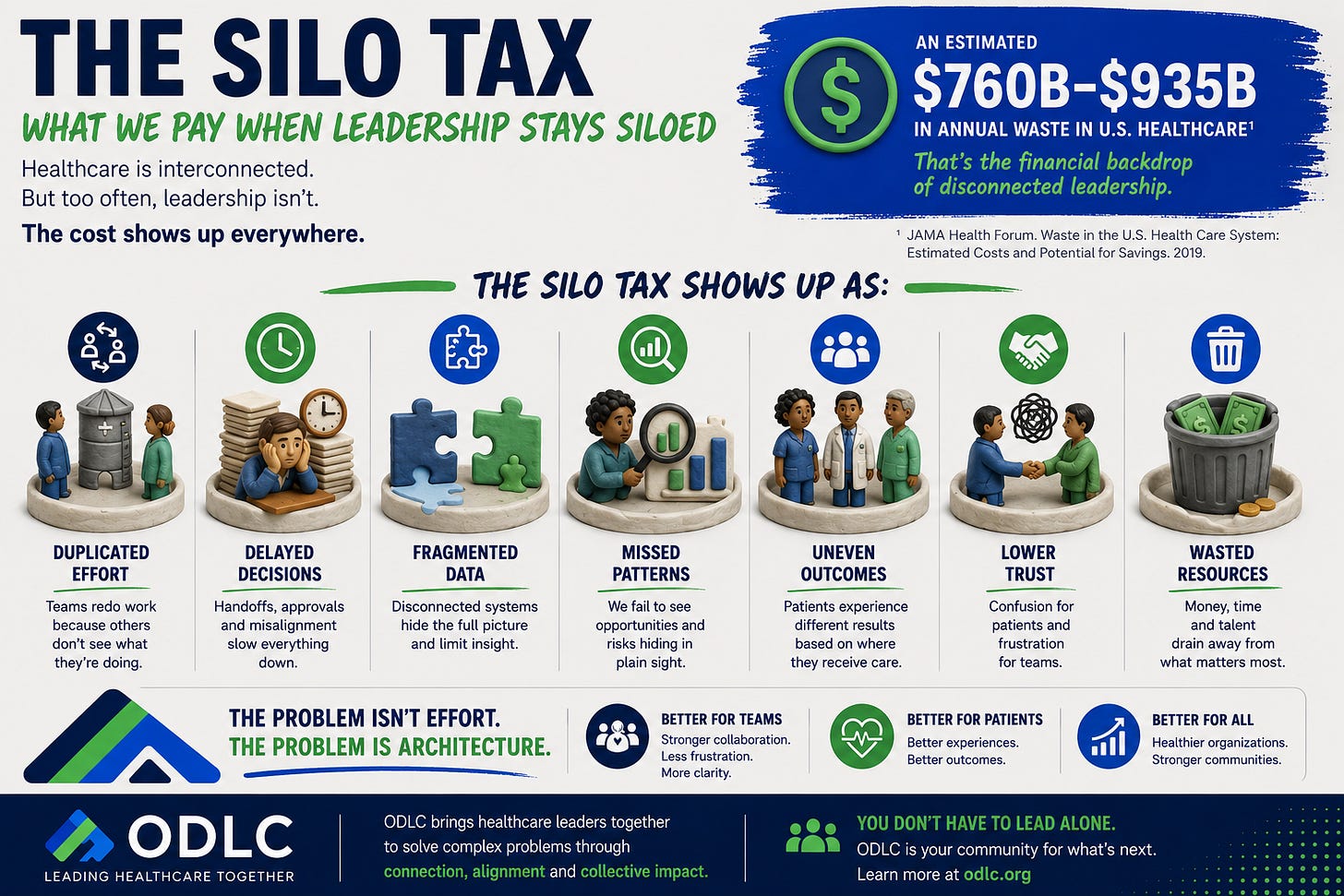
I think of it as the silo tax: the invisible price healthcare organizations pay when work that should be integrated is divided across teams, titles, departments, service lines, budgets, dashboards, and decision-making structures.
The silo tax shows up quietly at first. It shows up when the access team is trying to improve scheduling, but the clinical team is not at the table to explain why certain visit types require different workflows. It shows up when a quality dashboard identifies variation, but no one has connected that variation to geography, transportation, language, referral patterns, trust, or social need. It shows up when a health equity leader is asked to “weigh in” after the strategy has already been designed, instead of being built into the operating model from the beginning.
It also shows up when a med tech innovation is introduced as a product solution, but the implementation plan fails to account for culture, workflow, incentives, or the lived realities of the people expected to use it. It shows up when community engagement is celebrated externally, but internally, the insights from those communities never make it into the decisions that shape care delivery.
And perhaps most importantly, it shows up when leaders keep asking, “Who owns this?”
When the better question may be: What system is required for this to work?
The Problem Is Not Effort. The Problem Is Architecture.
One of the hardest truths in healthcare leadership is that effort does not automatically equal alignment. Some of the most exhausted teams I counsel are working incredibly hard within structures that were never designed to connect their work.
That is why siloed leadership is so costly. It allows organizations to mistake activity for strategy. A committee becomes a sign of progress. A dashboard becomes a sign of accountability. A pilot becomes a sign of innovation. A statement becomes a sign of commitment.
But if those efforts are not connected to decision-making, resource allocation, operational workflows, leadership accountability, and measurable outcomes, then the work remains vulnerable. It may be visible, but it is not yet built in.
And in today’s healthcare environment, built-in matters.
Leaders are being asked to improve quality, reduce variation, expand access, strengthen trust, manage cost, retain teams, respond to community need, implement new technologies, and navigate a political landscape that can make even mission-driven work feel more fragile.
This is exactly why silos are no longer just an inconvenience. They are a leadership risk.
Why This Matters Now
For years, many organizations treated equity, quality, access, workforce experience, innovation, and community health as adjacent lanes. Important lanes, yes. But still separate.
That separation may have felt manageable when the environment was less complex. But healthcare is now operating in a moment where the old separations no longer hold.
You cannot improve quality while ignoring the patients who experience worse outcomes. You cannot improve access without understanding the operational barriers that shape who gets care, when they get it, and how easily they can return. You cannot improve workforce culture while asking teams to absorb poorly designed systems with a smile.
You cannot deploy technology effectively without understanding trust, adoption, workflow, and the uneven conditions under which care is delivered. You cannot build healthier communities if community insights stay outside the rooms where strategy is actually made.
This is the leadership pivot in front of us: the next era of healthcare will not belong to the leaders with the most isolated expertise. It will belong to the leaders who can integrate expertise across boundaries.
The Leadership Shift: From Ownership to Integration
Many leaders have been trained to ask ownership questions: Who owns quality? Who owns access? Who owns equity? Who owns innovation? Who owns community engagement?
Ownership matters. But in complex systems, ownership alone is insufficient.
The more powerful leadership question is integration: How does this work connect? Where does this decision live? Who is missing from the conversation? What workflow will actually change? What data will tell us whether the change is working? What accountability structure will keep this from becoming another well-intended side project?
That shift may sound subtle, but it is not. It changes the leader’s job from managing a lane to building connective tissue.
Five Leadership Moves to Reduce the Silo Tax
1. Name the connected problem, not just the departmental problem.
If the issue is readmissions, access delays, surgical outcomes, patient trust, technology adoption, or workforce burnout, resist the urge to define it too narrowly. Ask what else is connected.
A scheduling issue may also be a transportation issue, a staffing issue, a referral issue, a communication issue, and a trust issue. A quality gap may also be an access gap. A workforce concern may also be an operational design problem.
The way a problem is named determines who gets invited to solve it.
2. Build the table before the solution.
Healthcare leaders often move quickly to action because the needs are urgent. But fast action without the right table can create more fragmentation.
Before launching the initiative, ask: Who understands the workflow? Who sees the data pattern? Who hears the patient story? Who controls the resources? Who will be expected to implement this? Who will experience the consequences if we get it wrong?
The right table does not have to be large. But it does need to be honest.
3. Treat equity as a performance signal, not a separate project.
In today’s landscape, some leaders may feel pressure to move equity work to the margins, rename it, or disconnect it from core operations. But variation in outcomes, access, experience, and trust is not peripheral to healthcare performance.
It is healthcare performance.
If a system works reliably for some patients and inconsistently for others, that is not a branding issue. That is a quality, safety, access, and leadership issue.
The goal is not to protect a word. The goal is to build systems that produce better care for more people, more reliably.
4. Stop letting dashboards substitute for decisions.
Data can reveal a gap, but data alone does not close it. A dashboard should not be the final product. It should be the beginning of a better leadership conversation.
When reviewing data, ask: What decision should this change? What workflow should this improve? What resource should this redirect? What assumption should this challenge? What accountability should this create?
If no decision changes after the data is reviewed, the dashboard may be informative, but it is not yet transformative.
5. Reward the integrators.
Every organization has people who naturally connect dots across teams. They notice when one department’s solution creates a problem for another department. They translate between clinical, operational, community, and executive realities. They can see the system, not just the assignment.
Those people are often underrecognized because their work does not always fit neatly into a single job description.
Find them. Support them. Promote them. Give them authority.
The Question for Leaders This Week
Look at one priority that has been slow to move. Not the easiest priority. The one that keeps resurfacing in meetings. The one that everyone agrees matters, but no one seems able to fully advance.
Now ask whether the work is being treated as a departmental problem when it is actually a connected system problem. Ask whether the people closest to the workflow, the data, the community, and the decision-making are connected early enough. Ask what the organization is currently paying in duplicated effort, delayed decisions, missed trust, or uneven outcomes because this work remains siloed.
That is the silo tax. And the bill is usually higher than leaders think.
Resource Connection
At ODLC, we believe the future of healthcare leadership requires more than individual excellence. It requires leaders who can connect strategy to operations, equity to quality, innovation to implementation, and mission to measurable action.
That is why our member community and Dynamize Health leadership resources are designed to help healthcare professionals move from isolated effort to shared leadership practice.
Through ODLC membership, leaders gain access to a national community of peers, practical leadership resources, and conversations designed to help organizations move beyond symbolic commitment and into durable systems change.
And through Dynamize Health, leaders and teams can explore advisory support, leadership development, and certificate-based learning experiences designed to strengthen execution, integration, and value-driven transformation.
As you have heard me assert over the past several years, the future of healthcare will not be limited by the amount of good work that exists. It will be limited by whether leaders can connect that work into systems that actually move.
