
Picture it: A health system spends four years building a community health partnership.
A single leader drove it – showing up at community centers and school health fairs, training primary care teams, learning which community stakeholders to call when the system’s credibility needed to be vouched for.
The programs worked.
Surgical referral gaps started to close. Community trust, painstakingly earned, was paying off in enrollment, in outcomes, in data that finally told a better story.
Then the leader leaves.
A year later, the partnership has quietly collapsed. The community partners stopped returning calls after the third new point of contact in twelve months. The clinical champions who came around after eighteen months of relationship-building have moved on to other priorities. The organization announces a new initiative.
New name. New hire.
No institutional memory of why the last one worked.
Sound familiar?
This scenario plays out across our field more often than we formally track. And it is not primarily a talent problem.
It is a design problem.
What we lose when leaders who carry equity, access, and community health leave a health system is rarely captured in any exit interview.
We lose the trust built with communities over years of consistent presence. We lose the clinical champions who took a long time to earn. We lose the institutional memory: who to call, how to navigate internal resistance, where the actual decision-making power sits when it isn’t on the org chart.
None of that is in a handbook.
Change the Frame
The conversation around workforce belonging in healthcare is largely framed as a recruitment and retention issue: how do we get diverse talent in, and how do we keep them?
That framing is too narrow.
When leaders doing equity-focused work leave, it is often because their work is structurally peripheral; present enough to signal commitment, absent enough to be cut when the political or financial climate shifts.
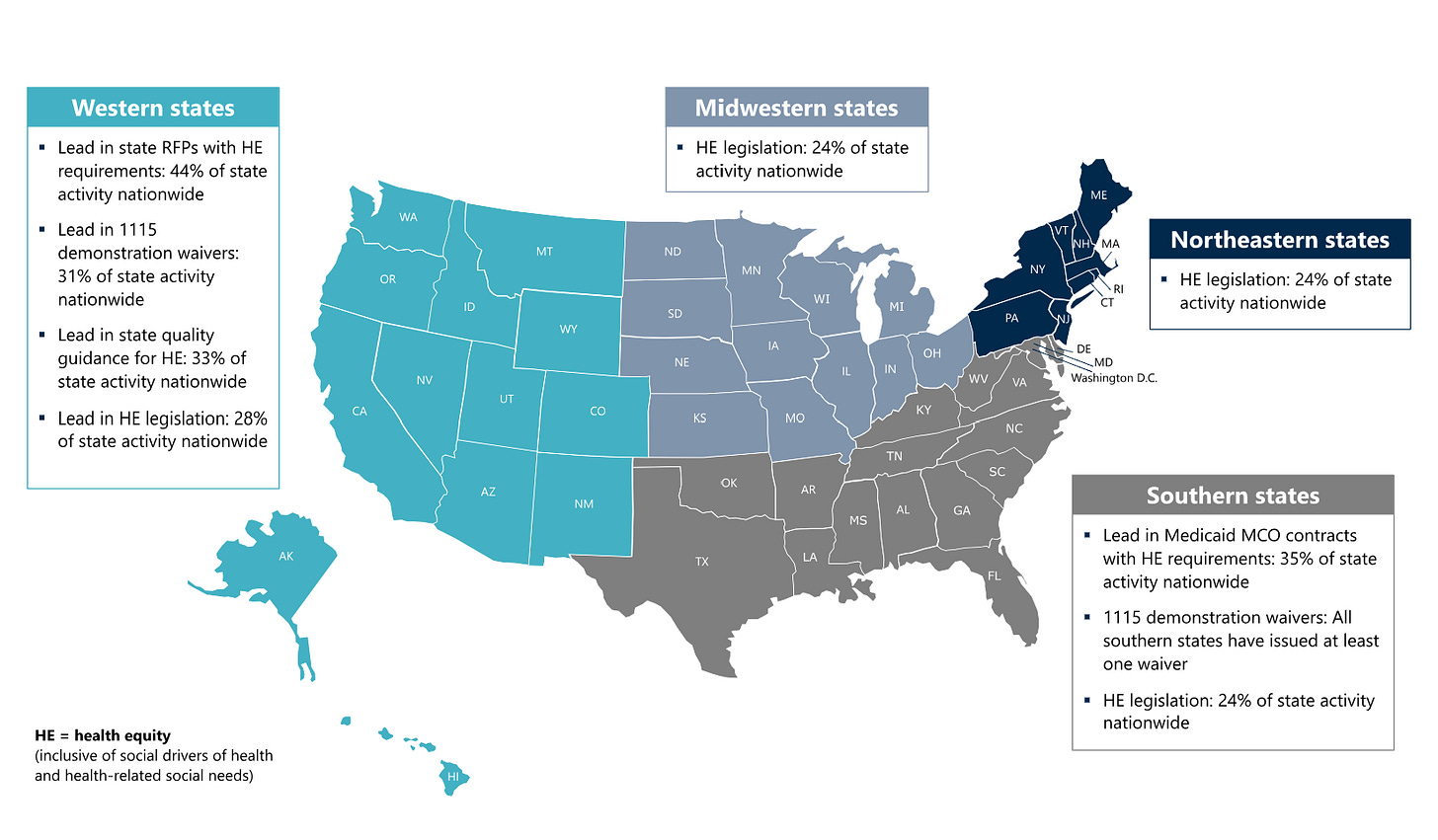
A HealthScape Advisors analysis published earlier this year found that states are largely staying the course on health equity policy, building resilience through embedded systems-level approaches. But inside individual health systems, that kind of stability is far less consistent.
The leaders feeling that inconsistency most acutely are often the ones the institution can least afford to lose.
Research on engagement makes the stakes concrete. Across industries, Gallup has found that managers account for a substantial share (70%) of the variance in employee engagement, underscoring what healthcare leaders already know from experience: the conditions people work in are shaped heavily by the leaders closest to the work.
People often leave conditions, not organizations.
For clinician leaders whose professional identity is tied to equitable care delivery, an institution that treats that work as peripheral sends a message that lands loud and clear.
A 2026 workforce analysis by VitalWorkLife found that 55% of healthcare workers are considering leaving their jobs this year, with 84% reporting they feel underappreciated. These numbers are not explained by workload and pay alone.
They reflect a leadership environment not designed to sustain people doing complex, relational, long-cycle work.
Equity-focused leaders live at the intersection of all three.
For organizations ready to examine this honestly, the Dynamize Health Equity Leadership Index offers a structured starting point – mapping not just where equity and community health programs exist, but whether the institutional conditions that make those programs sustainable are actually in place.
Translation to Practice
What does this mean operationally for the leaders in our network?
First: identify which equity-focused leaders in your organization are doing work with no structural support beneath it – no dedicated budget, no named governance home, no integration into quality dashboards.
These are the people most at risk when financial or political pressure builds.
And they are the last people whose departure gets attributed to the correct cause.
Second: treat the relational capital these leaders carry as institutional capital.
Map it deliberately.
The community partnerships they maintain. The clinical champions they’ve cultivated. The trust they hold in rooms the organization cannot easily enter on its own.
When these leaders leave, that capital does not transfer automatically. It requires intentional succession and knowledge-transfer infrastructure — built before the departure notice, not after.
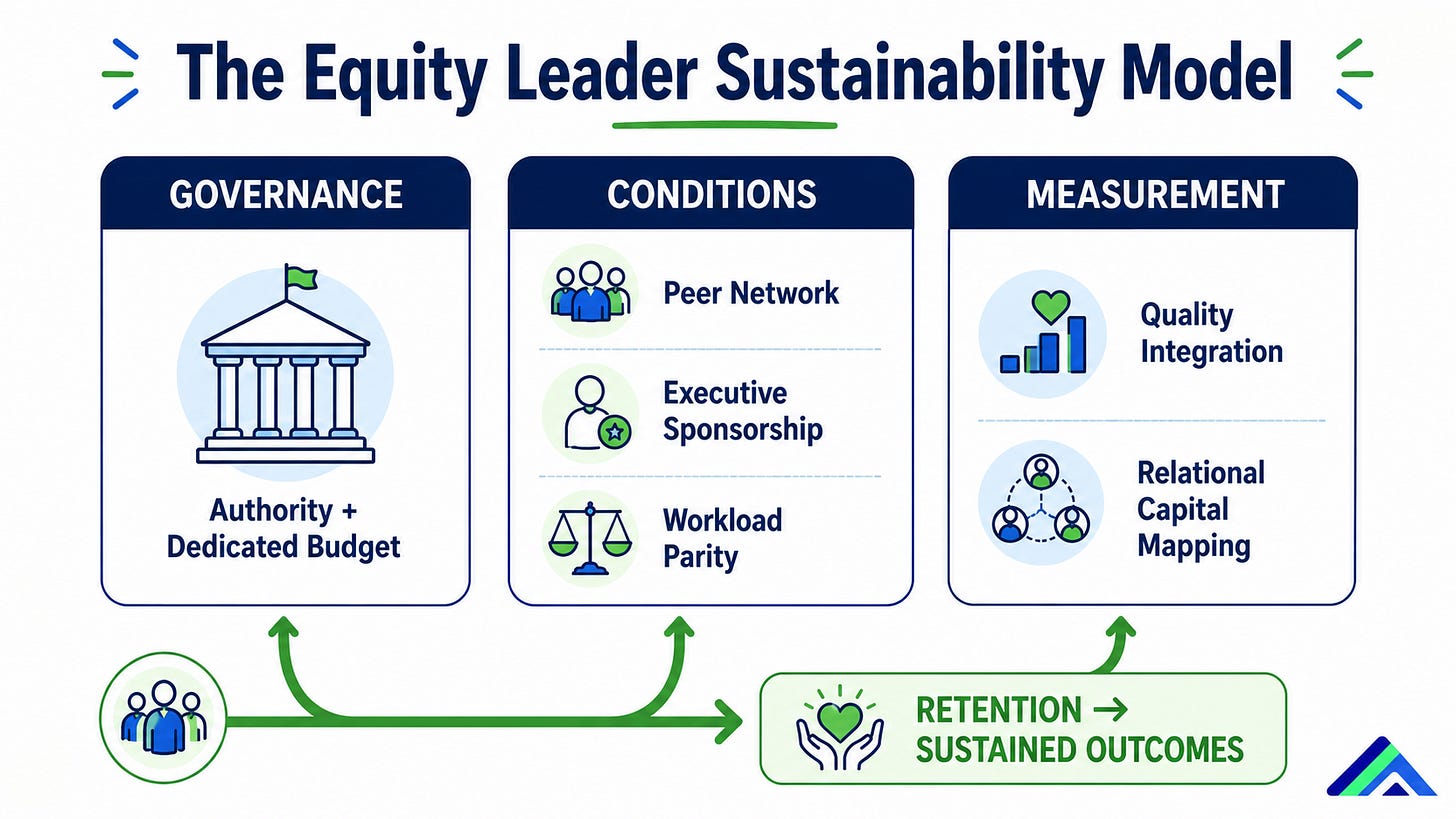
Third: build leadership conditions where equity-focused leaders feel they belong in the institution they are being asked to change.
That means specific, auditable commitments: peer community, executive sponsorship, workload parity, and a real seat in the rooms where operational decisions are made.
Not an advisory seat. A decision-making one.
The organizations that are getting this right are not necessarily the loudest ones. They’re the ones quietly designing conditions that make the work sustainable before they need to hire for the role a second time.
A Note to Our ODLC Community
To the leaders in our network holding this right now – those of you building belonging inside institutions that weren’t designed with you in mind, carrying community trust on behalf of systems still learning to earn it – we see you.
This work is exhausting.
It is also among the most consequential leadership work being done in healthcare today.
You are not doing it alone.
The ODLC community was built for exactly this: a space where leaders doing the hardest work don’t have to explain themselves before they can find the support they need.
The weight you’re carrying is real.
So is the network behind you.
The organizations that retain their equity-focused leaders will not just feel the difference in culture. They will see it in their outcomes data, in their community partnership stability, and in the quality metrics that actually matter to the patients we all came to serve.
What leaves when they leave is not just a person.
It is the community partnership no one formally owned, the clinical champion no one remembered to re-engage, the trust network no dashboard captured, and the hard-earned relationship the system never counted as an asset until it was gone.
Leadership Takeaways
Audit peripheral equity roles.
If equity-focused leaders in your organization carry significant relational capital with no structural backing – no budget line, no governance integration, no accountability structure – they are at retention risk. Identify them. Change the conditions before the exit interview.
Map relational capital before it walks out.
Community partnerships, clinical champions, and institutional trust networks built by equity leaders are organizational assets. Document them. Treat succession in these roles with the same rigor applied to any other critical position.
Connect belonging to outcomes.
When equity-focused leadership turnover is high, the downstream effects show up in quality metrics, community health partnership stability, and patient experience scores. Measure the connection. Present the case in the language of operational performance.
This week: ask the direct question.
Reach out to one equity-focused leader in your organization and ask honestly: what would make this work sustainable here? What does this institution need to do differently?
Then stay for the full answer.
Where to Go from Here
If this resonates, ODLC membership is where our network comes together to do exactly this – learn from each other, sharpen strategy, and lead with less isolation.
We’d love to have you at the table.
